Life Cycle
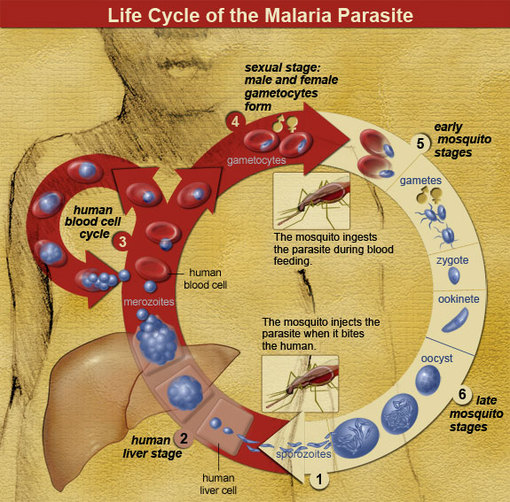
The life cycle of the malaria parasite is very specific and complex, and is very effective against humans. The life cycle begins when an uninfected mosquito bites an infected human and acquires the malaria parasite of the genus Plasmodium (1).
When an uninfected female mosquito bites an infected human, the female and male gametophytes of malaria enter the mosquito. These sexual haploid forms of the parasite are called the macrogametocyte (female) and the microgametocyte (male) (2). When they enter the gut of the mosquito, the mature microgametocyte flagellates quickly to the female macrogametocyte for fertilization. In this step, a diploid zygote is formed. These zygotes develop into active ookinetes within eighteen to twenty-four hours that bury into the midgut wall of the mosquito. When the ookinetes reach the extracellular space between the midgut epithelium and the basal lamina, they develop into oocysts.
The oocysts grow and divide after eight to fifteen days, and each division produces thousands of haploid sporozoites (3). These motile sporozoites travel to the salivary glands of the mosquito, and when the mosquito bites an uninfected human, the sporozoites in the salivary glands enter the human bloodstream, infecting the human and making it its host.
By traveling through the blood stream, the sporozoites enter the human liver with the help of thrombospondin-related anonymous proteins (TRAP) and an actin-myosin complex (2). When they enter the liver, they infect the liver cells, called hepatocytes, and develop into schizonts which contain 10,000-30,000 merozoites. The schizonts stay in the liver for about five to sixteen days, but sometimes they may remain dormant in the liver for years before the host starts developing symptoms.
The merozoites that are released into the bloodstream from the liver are contained inside host-cell derived merosomes. This way, the immune system of the host does not recognize the parasite as a foreign object. In the bloodstream, the merozoites infect the red blood cells by ligand receptors on the blood cell very quickly, about thirty seconds. This also reduces the chance for the immune system to recognize the merozoite because once they are in the red blood cell, they are unrecognizable. The parasite enters through with the help of an actin-myosin motor complex and TRAP, and creates a vacuole to isolate and seal itself from the cytoplasm of the red blood cell.
Within the red blood cell, the parasite grows reproduces asexually. Hemoglobin is the main food source for the parasite which is ingested into a food vacuole and degraded. The parasite also depends on anaerobic glycolysis. As the parasite grows and multiplies within the red cell, the membrane permeability and cytosolic composition of the host cell is modified. Each merozoite asexually produces 8-32 new merozoites. When division and reproduction is complete, the red blood cell bursts and is ruptured and destroyed (4). This step of the cycle causes the symptoms of the disease. As more and more merozoites are produced and released into the bloodstream, more erythrocytes become infected and killed by the parasite. Some merozoites in the erythrocyte develop into sexual forms, the gametocyte. When an uninfected mosquito bites the host and takes in these gametocytes, the life cycle starts all over again.(5)
When an uninfected female mosquito bites an infected human, the female and male gametophytes of malaria enter the mosquito. These sexual haploid forms of the parasite are called the macrogametocyte (female) and the microgametocyte (male) (2). When they enter the gut of the mosquito, the mature microgametocyte flagellates quickly to the female macrogametocyte for fertilization. In this step, a diploid zygote is formed. These zygotes develop into active ookinetes within eighteen to twenty-four hours that bury into the midgut wall of the mosquito. When the ookinetes reach the extracellular space between the midgut epithelium and the basal lamina, they develop into oocysts.
The oocysts grow and divide after eight to fifteen days, and each division produces thousands of haploid sporozoites (3). These motile sporozoites travel to the salivary glands of the mosquito, and when the mosquito bites an uninfected human, the sporozoites in the salivary glands enter the human bloodstream, infecting the human and making it its host.
By traveling through the blood stream, the sporozoites enter the human liver with the help of thrombospondin-related anonymous proteins (TRAP) and an actin-myosin complex (2). When they enter the liver, they infect the liver cells, called hepatocytes, and develop into schizonts which contain 10,000-30,000 merozoites. The schizonts stay in the liver for about five to sixteen days, but sometimes they may remain dormant in the liver for years before the host starts developing symptoms.
The merozoites that are released into the bloodstream from the liver are contained inside host-cell derived merosomes. This way, the immune system of the host does not recognize the parasite as a foreign object. In the bloodstream, the merozoites infect the red blood cells by ligand receptors on the blood cell very quickly, about thirty seconds. This also reduces the chance for the immune system to recognize the merozoite because once they are in the red blood cell, they are unrecognizable. The parasite enters through with the help of an actin-myosin motor complex and TRAP, and creates a vacuole to isolate and seal itself from the cytoplasm of the red blood cell.
Within the red blood cell, the parasite grows reproduces asexually. Hemoglobin is the main food source for the parasite which is ingested into a food vacuole and degraded. The parasite also depends on anaerobic glycolysis. As the parasite grows and multiplies within the red cell, the membrane permeability and cytosolic composition of the host cell is modified. Each merozoite asexually produces 8-32 new merozoites. When division and reproduction is complete, the red blood cell bursts and is ruptured and destroyed (4). This step of the cycle causes the symptoms of the disease. As more and more merozoites are produced and released into the bloodstream, more erythrocytes become infected and killed by the parasite. Some merozoites in the erythrocyte develop into sexual forms, the gametocyte. When an uninfected mosquito bites the host and takes in these gametocytes, the life cycle starts all over again.(5)
Pathophysiology
When newly formed merozoites are released from ruptured erythrocytes, many unknown substances and waste are also released that are toxic to the body, such as glycosylphosphatidylinositol (GPI). The GPI activates macrophages that secrete cytokines and inflammatory mediators. These inflammatory mediators include tumor necrosis factor, interferon- ϒ, interlukin-1, Iymphotoxin and nitric oxide (6). This GPI toxin causes may cytokines to be released, which are cell-signaling protein molecules. This response to the toxin causes many of the flu-like symptoms associated with malaria.
The plasmodial DNA of malaria also causes high inflammatory response and release cytokines. The hemozoin pigment present in the DNA interacts with TLR9 in the body that results in the release of the cytokines. This then induces COX-2, an enzyme that stimulates inflammation and pain, causing fever. This process is shown below.
The plasmodial DNA of malaria also causes high inflammatory response and release cytokines. The hemozoin pigment present in the DNA interacts with TLR9 in the body that results in the release of the cytokines. This then induces COX-2, an enzyme that stimulates inflammation and pain, causing fever. This process is shown below.
The pathophysiology described above usually relates to flu-like symptoms. However, there is also a pathophysiology of malaria causing severe malaria. Severe malaria is associated with a specific type of malaria called P. falciparum. P. falciparum can infect any age of erythrocyte, causing the malaria parasite to grow exponentially in the host. This causes 20-30% of the red blood cells to become infected.
If the release of cytokines is too high in severe malaria, it can result in many complications such as enhanced lactate production, poor circulation and severe tissue hypoxia, red cell deformability, reduced gluconeogenesis, cardiac insufficiency, cerebral malaria, and activation of leukocytes and platelets, causing greater coagulation of the blood (6).
Structural changes can result in severe malaria. These include:
· Cytoadherence- red blood cells already affected with malaria adhere to the capillary and postcapillary venular endothelium.
· Sequestration-caused by cytoadherence, infected erythrocytes build up in the organs. This provides a better environment for the parasite in which they can grow to avoid clearance by the spleen and be unrecognized by the immune system.
· Rosetting- infected erythrocytes adhere to uninfected erythrocytes, causing formation of rosettes.
If the release of cytokines is too high in severe malaria, it can result in many complications such as enhanced lactate production, poor circulation and severe tissue hypoxia, red cell deformability, reduced gluconeogenesis, cardiac insufficiency, cerebral malaria, and activation of leukocytes and platelets, causing greater coagulation of the blood (6).
Structural changes can result in severe malaria. These include:
· Cytoadherence- red blood cells already affected with malaria adhere to the capillary and postcapillary venular endothelium.
· Sequestration-caused by cytoadherence, infected erythrocytes build up in the organs. This provides a better environment for the parasite in which they can grow to avoid clearance by the spleen and be unrecognized by the immune system.
· Rosetting- infected erythrocytes adhere to uninfected erythrocytes, causing formation of rosettes.
The protein PfEMP1 mediates adhesion of infected red blood cells to the endothelium and the uninfected red blood cells. They bind to adhesion receptors expressed on endothelial cells and receptor 1, CD31, and heparin sulfate-like glycosaminoglycans found on uninfected red blood cells.
Sometimes, an erythrocyte mass becomes rigid when they adhere together. This is caused by several mechanisms, such as change in the phospholipid bilayer and inhibition of the Na+/K+ pump on the erythrocyte membrane (6). This rigidity leads to splenic clearance and anemia, the loss of red blood cells.
Sometimes, an erythrocyte mass becomes rigid when they adhere together. This is caused by several mechanisms, such as change in the phospholipid bilayer and inhibition of the Na+/K+ pump on the erythrocyte membrane (6). This rigidity leads to splenic clearance and anemia, the loss of red blood cells.
Symptoms of Malaria
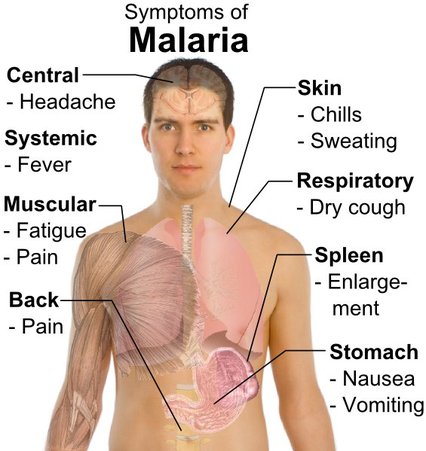
The symptoms of malaria are caused by the merozoites rupturing the erythrocytes of the host when they reproduce. When the infected blood cell bursts, toxins and waste produced in the cell from the parasite are released into the bloodstream, along with the new merozoites. Various macrophages recognize these foreign toxins, causing the many symptoms such as fever. Malaria is most common in tropical and subtropical areas due to the warm climate, rainfall, and stagnant water which create an ideal habitat for mosquito larvae.
The symptoms begin about 8-25 days after the host has been infected. Symptoms are common to symptoms of the flu, which includes fever, headache, vomiting, and joint pain. If not treated early, malaria can become fatal and complications can occur. Although these symptoms are life threatening, malaria is a treatable disease. If addressing symptoms of malaria, physicians who are not used to treating malaria may misdiagnose with the flu. Suspicion of malaria must be handled appropriately through proper diagnosis by the microscopic examination of blood using blood films.
The symptoms begin about 8-25 days after the host has been infected. Symptoms are common to symptoms of the flu, which includes fever, headache, vomiting, and joint pain. If not treated early, malaria can become fatal and complications can occur. Although these symptoms are life threatening, malaria is a treatable disease. If addressing symptoms of malaria, physicians who are not used to treating malaria may misdiagnose with the flu. Suspicion of malaria must be handled appropriately through proper diagnosis by the microscopic examination of blood using blood films.
Levels of Disease
Uncomplicated Malaria: This level of the disease includes symptoms that are similar to the common flu. These symptoms include fever, sweats, chills, headache, vomiting, and body aches. Some common recognizable physical changes include weakness, enlarged spleen or liver, mild jaundice, increased respiration, and perspiration. Microscopy can detect parasites in the blood, or decrease in blood platelets can diagnose malaria. Individuals often experience malaria attacks which include three stages: a cold stage (sensation of cold, shivering), a hot stage (fever, headaches, vomiting; seizures in young children), and finally a sweating stage (sweats, return to normal temperature, tiredness). Uncomplicated malaria can be associated with all five types of malaria.
Severe Malaria: Results due to organ failure usually caused by P. falciparum. Symptoms indicative of severe malaria include severe anemia due to hemolysis (destruction of the red blood cells), hemoglobinuria (hemoglobin in the urine) due to hemolysis , acute respiratory distress syndrome, abnormalities in blood coagulation, low blood pressure caused by cardiovascular collapse, acute kidney failure, hyperparasitemia, where more than 5% of the red blood cells are infected by malaria parasites, metabolic acidosis, and hypoglycemia (low blood glucose). These symptoms affect the liver, heart, lungs, brain, and many of the vital systems of the body.
Severe Malaria: Results due to organ failure usually caused by P. falciparum. Symptoms indicative of severe malaria include severe anemia due to hemolysis (destruction of the red blood cells), hemoglobinuria (hemoglobin in the urine) due to hemolysis , acute respiratory distress syndrome, abnormalities in blood coagulation, low blood pressure caused by cardiovascular collapse, acute kidney failure, hyperparasitemia, where more than 5% of the red blood cells are infected by malaria parasites, metabolic acidosis, and hypoglycemia (low blood glucose). These symptoms affect the liver, heart, lungs, brain, and many of the vital systems of the body.
References
1. http://www.infection-research.de/infectious_diseases/malaria/
2. http://www.malariasite.com/malaria/LifeCycle.htm
3. http://www.niaid.nih.gov/topics/malaria/pages/lifecycle.aspx
4. http://content.karger.com/ProdukteDB/Katalogteile/isbn3_8055/_73/_76/CI80-Fujioka.pdf
5. http://www.youtube.com/watch?v=859YQcqYPko
6. http://www.malariasite.com/malaria/Evolution.htm
7. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1224522/
8. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3375727/
9. http://www.nejm.org/doi/full/10.1056/NEJMcp0803572
2. http://www.malariasite.com/malaria/LifeCycle.htm
3. http://www.niaid.nih.gov/topics/malaria/pages/lifecycle.aspx
4. http://content.karger.com/ProdukteDB/Katalogteile/isbn3_8055/_73/_76/CI80-Fujioka.pdf
5. http://www.youtube.com/watch?v=859YQcqYPko
6. http://www.malariasite.com/malaria/Evolution.htm
7. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1224522/
8. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3375727/
9. http://www.nejm.org/doi/full/10.1056/NEJMcp0803572
