Types of Malaria
Plasmodium is the genus of the protist which infects humans and other animals with malaria. There are five species of Plasmodium that can infect and be transmitted by humans. These species include P. falciparum, P. malariae, P. ovale, P. vivax and P. knowlesi. The majority of malaria cases that result in deaths are due to P. falciparum which is also the most common species identified. P. malariae, P. ovale, and P. vivax cause a much milder form of malaria and rarely result in death.
Prevalence of Malaria
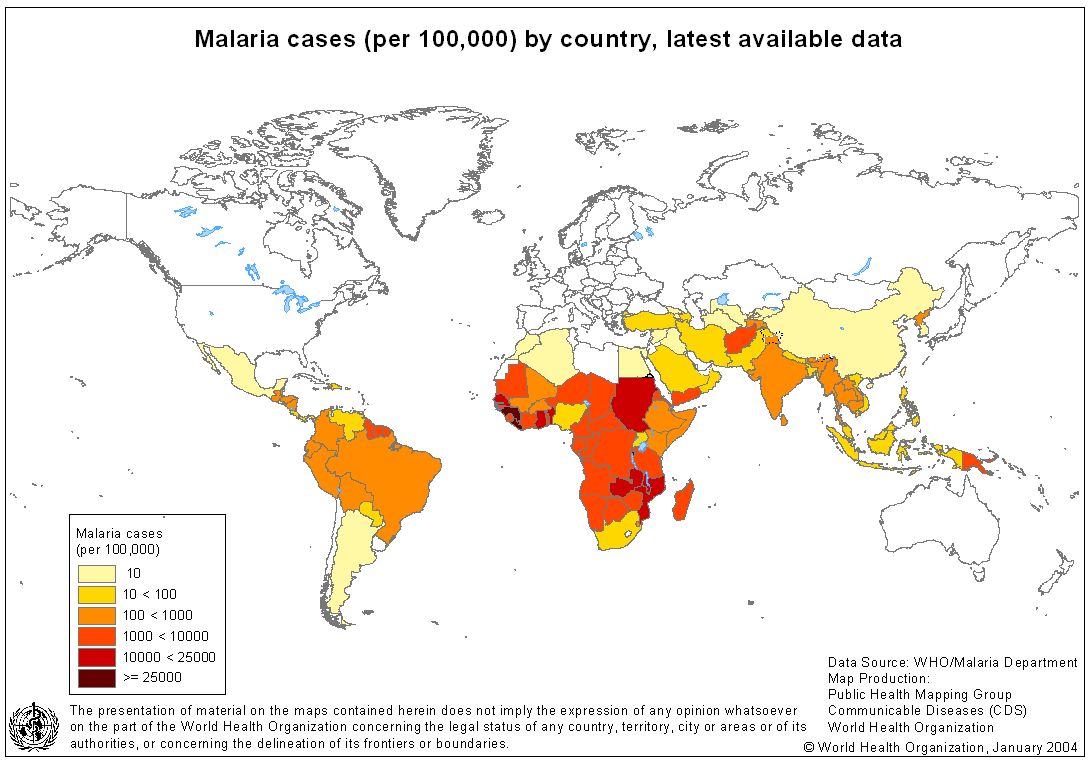
Malaria is most common in tropical and subtropical areas due to the warm climate, rainfall, and stagnant water which create an ideal habitat for mosquito larvae. Malaria is the world’s most important parasitic disease which affects 300-500 million people each year. Approximately 40% of the world’s population is affected with malaria with 1.5-2.7 million deaths occurring each year.
Prevention
Malaria prophylaxis is a preventative treatment for malaria. Many travelers will often practice malaria prophylaxis in preparation to travel to a foreign country where malaria is popular. This is accomplished by taking various oral medications at different times prior to departing to the country, while in the country, and after returning from the country. Medications involved in malaria prophylaxis are chloroquine, doxycyline, mefloquine, primaquine, and a combination of atovaquone and proguanil. As mentioned in the following section, these drugs are often used to treat malaria as well.
Diagnosis
Although symptoms of malaria are life threatening, malaria is a treatable disease. If addressing symptoms of malaria, physicians who are not used to treating malaria may often misdiagnose individuals with the flu. Suspicion of malaria must be handled appropriately through proper diagnostic techniques. Common laboratory assays which can diagnose malaria include microscopy, antigen detection, and molecular diagnosis. Malaria must be recognized early in order to fully treat the symptoms as well as prevent spreading. Those with cases treated early can expect a full recovery; however, severe cases of malaria exist where the disease progresses rapidly and can result in death within hours or days.
Laboratory Assays
Microscopy techniques are the most common form of detecting malaria. A “blood smear” is used by placing drop of the patient’s blood on a microscope slide. The parasites are then stained, and can be detected under the microscope to confirm infection. Antigen detection of malaria has been recently established by the use of rapid diagnostic tests. These tests are beneficial in areas that do not have access to microscopy and provide quick results to aid in a faster diagnosis. These rapid diagnostic tests work by taking a blood sample from the patient and placing it on a test card allowing detection of a specific biosensor. Results are given in just 15 minutes. An advantage to these tests include the indication of a rapid result, however, disadvantages include the cost and accuracy. Molecular diagnosis includes the detection of parasite nucleic acid through the use of polymerase chain reaction. This technique is commonly used for patients who may be acutely ill with the disease, as results are not given in a timely matter. This test is very sensitive and can confidently confirm the malaria infection.
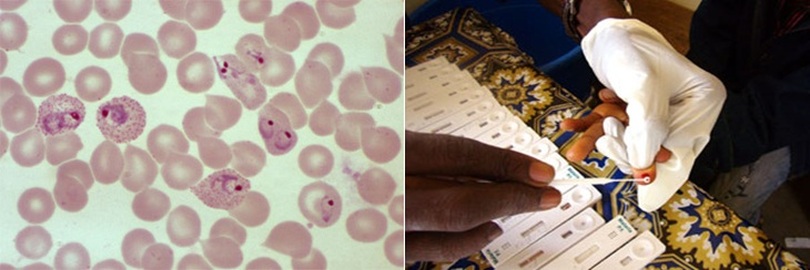
Blood smear of a patient diagosed malaria. Rapid diagnosis test used to determine malaria infection.
Treatment
The type of treatment for malaria varies depending on multiple factors. These factors include the species of the Plasmodium parasite which has infected the host, the severity of the disease, the age of the patient, whether or not the patient is pregnant, and the drug susceptibility of the infecting parasites. The location where the infection was acquired also determines what type of treatment can be administered. There are a variety of parasites that are drug resistant because of the location of the parasites.
Majority of malaria cases can be treated with oral medications; however, severe cases of malaria may require intravenous drug treatment. The most common oral medications include chloroquine (Aralen), Quinine sulfate (Qualaquin), hydroxychloroquine (Plaquenil), mefloquine, and a combination of atovaquone and proguanil (Malarone).
Chloroquine (Aralen) is the drug of choice to treat all species of malaria. While the drug can inhibit certain enzymes, its effect is believed to result, its interaction with DNA. However, the mechanism of plasmodicidal action of chloroquine is not completely certain. Chloroquine is rapidly and almost completely absorbed from the gastrointestical tract, and only a small proportion of the administered dose is found in the stool. Approximately 55% of the drug in the plasma is bound to nondiffusable plasma constituents. Excretion of chloroquine is quite slow, but it is increased by acidification of the urine. It is also deposited in the tissues in considerable amounts.
Physicians use chloroquine to treat malaria, as well as to prevent it. To prevent malaria, chloroquine is taken once, 1 to 2 weeks prior to traveling to an area where malaria is present, weekly while you are in the area, and weekly for 4 weeks after departing from the area. To treat malaria, the chloroquine is taken in intervals, increasing the dosage each time. The effectiveness of the medication depends on the location where the disease was acquired. Common side effects include nausea, diarrhea, dizziness, blurred vision, vivid dreams, headaches, and itching of the skin.
Quinine sulfate (qualaquin) not only treats malaria, but also prevents the development of malaria parasites in the blood, specifically in Plasmodium falciparum malaria. It is also the first ever chemotherapeutic agent to be identified and used against the malaria parasite. To treat malaria, quinine can be taken alone for 3 to 7 days, but it is more common to take quinine along with 1 of 3 other medications, doxycycline, tetracycline, or clindamycin, for 7 days. The combination of quinine with various medications is desired for chloroquine-resistant malaria, where chloroquine is no longer effective against the malaria parasite. When swallowed, quinine is absorbed readily from the upper small intestine, and in plasma, it is bound to the plasma protein. In severe malaria, when given in therapeutic doses, increased protein binding prevents any possible quinine toxicity. Many people who have taken this drug have reported side effects that are slim to none; however, side effects are still possible. Common side effects include nausea, blurred vision, headache, and ringing in the ears.
Hydroxychloroquine (Plaquenil) is classified as an anti-malarial drug. It is similar to chloroquine, and is useful in treating several forms of malarial. It is a suppressive treatment and treats acute attacks of malaria due to Plasmodium vivax, P. malariae, P. ovale, and susceptible strains of P. falciparum. Hydroxychloroquine does not prevent relapses in patients against vivax or malariae strains because it is not effective against exo-erythrocytic forms of the parasite. This drug may prevent malaria parasites from metabolizing hemoglobin in human red blood cells. Hydroxychloroquine should only be used in pregnant women for malaria prophylaxis or treatment. Side effects include irritability, headache, weakness, hair lightening or lass, nausea, muscle pain, and rash and itching.
Mefloquine prevents the development of malaria parasites in the blood by acting against malarial parasites at the erythrocytic phase. Mefloquine works by destroying the parasite after it is released from the liver into the blood; however, it does not destroy Plasmodium (P.) vivax or P. ovale parasites that may remain in the liver. Mefloquine is also used to both treat and prevent malaria with an emphasis on preventing the disease. To prevent malaria, mefloquine is to be taken 1 to 3 weeks before the individual travels to an area where malaria is present, then weekly while the individual stays in the area, and finally weekly for 4 weeks after the individual leaves. Side effects include nausea and diarrhea, dizziness, sleep disturbances (vivid dreams), and headaches.
Malarone is a combination of atovaquone and proguanil hydrochloride medications used to stop the development of parasites in the blood that cause malaria. Many physicians use Malarone to treat patients with malaria in areas that have chloroquine-resistant or other resistant strains. The constituents of Malarone, atovaquone and proguanil hydrochloride, interfere with two different pathways involved in the biosynthesis of pyrimidines required for nucleic acid replication. Atocaquone is a selective inhibitor of parasite mitochondrial electron transport. Proguanil hydrochloride primarily exerts its effect by means of the metabolite sycloguanil, a dihydrofolate reductase inhibitor. Inhibition of dihydrofolate reductase in the malaria parasite disrupts deoxythymidylate synthesis. Common side effects of Malarone include headache, stomach pains, nausea, vomiting, mouth ulcers, and vivid dreams. An individual should not take Malarone if a kidney disease is present, and a creatinine clearance test may be needed to make sure the kidneys are functioning properly before taking Malarone.
Majority of malaria cases can be treated with oral medications; however, severe cases of malaria may require intravenous drug treatment. The most common oral medications include chloroquine (Aralen), Quinine sulfate (Qualaquin), hydroxychloroquine (Plaquenil), mefloquine, and a combination of atovaquone and proguanil (Malarone).
Chloroquine (Aralen) is the drug of choice to treat all species of malaria. While the drug can inhibit certain enzymes, its effect is believed to result, its interaction with DNA. However, the mechanism of plasmodicidal action of chloroquine is not completely certain. Chloroquine is rapidly and almost completely absorbed from the gastrointestical tract, and only a small proportion of the administered dose is found in the stool. Approximately 55% of the drug in the plasma is bound to nondiffusable plasma constituents. Excretion of chloroquine is quite slow, but it is increased by acidification of the urine. It is also deposited in the tissues in considerable amounts.
Physicians use chloroquine to treat malaria, as well as to prevent it. To prevent malaria, chloroquine is taken once, 1 to 2 weeks prior to traveling to an area where malaria is present, weekly while you are in the area, and weekly for 4 weeks after departing from the area. To treat malaria, the chloroquine is taken in intervals, increasing the dosage each time. The effectiveness of the medication depends on the location where the disease was acquired. Common side effects include nausea, diarrhea, dizziness, blurred vision, vivid dreams, headaches, and itching of the skin.
Quinine sulfate (qualaquin) not only treats malaria, but also prevents the development of malaria parasites in the blood, specifically in Plasmodium falciparum malaria. It is also the first ever chemotherapeutic agent to be identified and used against the malaria parasite. To treat malaria, quinine can be taken alone for 3 to 7 days, but it is more common to take quinine along with 1 of 3 other medications, doxycycline, tetracycline, or clindamycin, for 7 days. The combination of quinine with various medications is desired for chloroquine-resistant malaria, where chloroquine is no longer effective against the malaria parasite. When swallowed, quinine is absorbed readily from the upper small intestine, and in plasma, it is bound to the plasma protein. In severe malaria, when given in therapeutic doses, increased protein binding prevents any possible quinine toxicity. Many people who have taken this drug have reported side effects that are slim to none; however, side effects are still possible. Common side effects include nausea, blurred vision, headache, and ringing in the ears.
Hydroxychloroquine (Plaquenil) is classified as an anti-malarial drug. It is similar to chloroquine, and is useful in treating several forms of malarial. It is a suppressive treatment and treats acute attacks of malaria due to Plasmodium vivax, P. malariae, P. ovale, and susceptible strains of P. falciparum. Hydroxychloroquine does not prevent relapses in patients against vivax or malariae strains because it is not effective against exo-erythrocytic forms of the parasite. This drug may prevent malaria parasites from metabolizing hemoglobin in human red blood cells. Hydroxychloroquine should only be used in pregnant women for malaria prophylaxis or treatment. Side effects include irritability, headache, weakness, hair lightening or lass, nausea, muscle pain, and rash and itching.
Mefloquine prevents the development of malaria parasites in the blood by acting against malarial parasites at the erythrocytic phase. Mefloquine works by destroying the parasite after it is released from the liver into the blood; however, it does not destroy Plasmodium (P.) vivax or P. ovale parasites that may remain in the liver. Mefloquine is also used to both treat and prevent malaria with an emphasis on preventing the disease. To prevent malaria, mefloquine is to be taken 1 to 3 weeks before the individual travels to an area where malaria is present, then weekly while the individual stays in the area, and finally weekly for 4 weeks after the individual leaves. Side effects include nausea and diarrhea, dizziness, sleep disturbances (vivid dreams), and headaches.
Malarone is a combination of atovaquone and proguanil hydrochloride medications used to stop the development of parasites in the blood that cause malaria. Many physicians use Malarone to treat patients with malaria in areas that have chloroquine-resistant or other resistant strains. The constituents of Malarone, atovaquone and proguanil hydrochloride, interfere with two different pathways involved in the biosynthesis of pyrimidines required for nucleic acid replication. Atocaquone is a selective inhibitor of parasite mitochondrial electron transport. Proguanil hydrochloride primarily exerts its effect by means of the metabolite sycloguanil, a dihydrofolate reductase inhibitor. Inhibition of dihydrofolate reductase in the malaria parasite disrupts deoxythymidylate synthesis. Common side effects of Malarone include headache, stomach pains, nausea, vomiting, mouth ulcers, and vivid dreams. An individual should not take Malarone if a kidney disease is present, and a creatinine clearance test may be needed to make sure the kidneys are functioning properly before taking Malarone.
Various medications used to treat and prevent malaria.
Prognosis
The prognosis of malaria is generally good as infected individuals can expect a full recovery. Although there is a positive outlook ahead, the severity of the disease and geographical location also plays an important role. Majority of patients with uncomplicated malaria see improvements within just two days of treatment. Patients with severe malaria carry a poor prognosis depending on how fast physicians were able to treat the disease. Severe malaria tends to have a high mortality rate, but if caught in time, the disease can be cured.
References
1. http://www.cdc.gov/malaria/diagnosis_treatment/index.html
2. http://www.mayoclinic.com/health/malaria/DS00475/DSECTION=treatments-and-drugs
3. http://www.medicinenet.com/malaria/page5.htm
4. http://www.infectionlandscapes.org/2011/04/malaria-part-4-landscape.html
5. http://www.nobelprize.org/educational/medicine/malaria/readmore/global.html
6. http://www.cdc.gov/malaria/diagnosis_treatment/clinicians2.html
7. http://www.mcwhealthcare.com/medicines_drugs/antimalarial_exporter_manufacturer.htm
8. http://www.webmd.com/a-to-z-guides/quinine-sulfate-for-malaria
9. http://www.medicinenet.com/hydroxychloroquine/article.htm
10. http://bodyandhealth.canada.com/drug_info_details.asp?brand_name_id=4230&rot=4
11. http://www.webmd.com/a-to-z-guides/malarone-for-malaria
12. http://dailymed.nlm.nih.gov/dailymed/archives/fdaDrugInfo.cfm?archiveid=12058
13. http://www.webmd.com/a-to-z-guides/chloroquine-for-malaria
14. http://www.drugs.com/condition/malaria-prophylaxis.html
15. http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-3-infectious-diseases-related-to-travel/malaria.htm
16. http://mount-kinabalu-borneo.com/blog/wp-content/uploads/2006/12/chloro250mg.jpg
17. http://deskofbrian.com/wp-content/uploads/primaquine.jpg
18. http://www.msf.org.uk/UploadedImages/6b6b95b9-e34a-4083-bd00-7067c19da2e6.jpg
19. http://health.howstuffworks.com/diseases-conditions/infectious/malaria1.htm
2. http://www.mayoclinic.com/health/malaria/DS00475/DSECTION=treatments-and-drugs
3. http://www.medicinenet.com/malaria/page5.htm
4. http://www.infectionlandscapes.org/2011/04/malaria-part-4-landscape.html
5. http://www.nobelprize.org/educational/medicine/malaria/readmore/global.html
6. http://www.cdc.gov/malaria/diagnosis_treatment/clinicians2.html
7. http://www.mcwhealthcare.com/medicines_drugs/antimalarial_exporter_manufacturer.htm
8. http://www.webmd.com/a-to-z-guides/quinine-sulfate-for-malaria
9. http://www.medicinenet.com/hydroxychloroquine/article.htm
10. http://bodyandhealth.canada.com/drug_info_details.asp?brand_name_id=4230&rot=4
11. http://www.webmd.com/a-to-z-guides/malarone-for-malaria
12. http://dailymed.nlm.nih.gov/dailymed/archives/fdaDrugInfo.cfm?archiveid=12058
13. http://www.webmd.com/a-to-z-guides/chloroquine-for-malaria
14. http://www.drugs.com/condition/malaria-prophylaxis.html
15. http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-3-infectious-diseases-related-to-travel/malaria.htm
16. http://mount-kinabalu-borneo.com/blog/wp-content/uploads/2006/12/chloro250mg.jpg
17. http://deskofbrian.com/wp-content/uploads/primaquine.jpg
18. http://www.msf.org.uk/UploadedImages/6b6b95b9-e34a-4083-bd00-7067c19da2e6.jpg
19. http://health.howstuffworks.com/diseases-conditions/infectious/malaria1.htm

{kind=link}
{kind=link}
{kind=link}